How Fiber Affects Weight Regulation
Consumption of carbohydrates and dietary fiber protects against obesity (Slavin, 2005). Examining the relationship between dietary fiber intake and body weight, however, is difficult due to the struggle to define dietary fiber and agree on recommended intake levels.
In 2002, the Dietary Reference Intakes (DRIs) published definitions for fiber (DRIs, 2002). Dietary fiber consists of nondigestible carbohydrates and lignin that are intrinsic and intact in plants. Functional fiber describes the isolated nondigestible carbohydrates that have beneficial physiological effects in humans. Total fiber is the sum of dietary fiber and functional fiber. Nondigestible means not digested and absorbed in the human small intestine. Fibers can be fermented in the large intestine or can pass through the digestive tract unfermented.
Sufficient data were not available to determine an Estimated Average Requirement (EAR), and thus calculate a Recommended Dietary Allowance (RDA) for Total Fiber, so an Adequate Intake (AI) was developed instead. The AI for fiber is based on the median fiber intake level observed to achieve the lowest risk of coronary heart disease (CHD): 14 g dietary fiber/1,000 kcal intake. A Tolerable Upper Intake Level (UL) was not set for dietary fiber or functional fiber. Nutrition Facts labels use 25 g/day of dietary fiber for a 2,000 kcal/day diet or 30 g/day for a 2,500 kcal/day diet as goals for American intake.
The solubility of fiber was originally thought to determine physiological properties, with soluble fiber linked to cholesterol lowering and insoluble fiber linked to laxation effects. The Dietary Reference Intake (DRI) Committee recommended development of new fiber descriptors, such as viscosity and fermentability, which may more accurately describe physiologic effects. Manufacturers are still allowed to list total dietary fiber, soluble fiber, and insoluble fiber on the Nutrition Facts panel. DRIs recommend daily dietary fiber consumption of 14 g/1,000 kcal or 25 g for adult women and 38 g for adult men. This amount is based on epidemiological studies showing protection against cardiovascular disease.
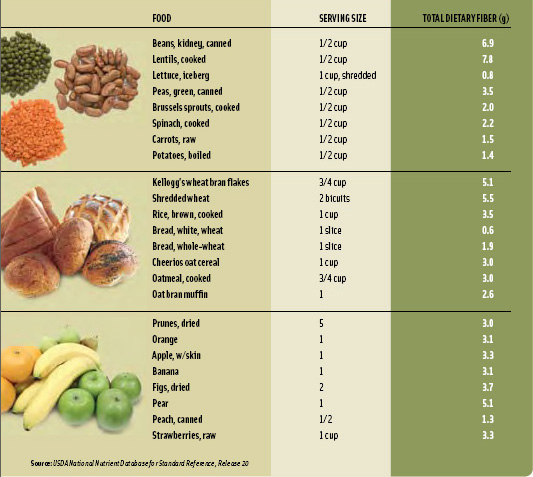
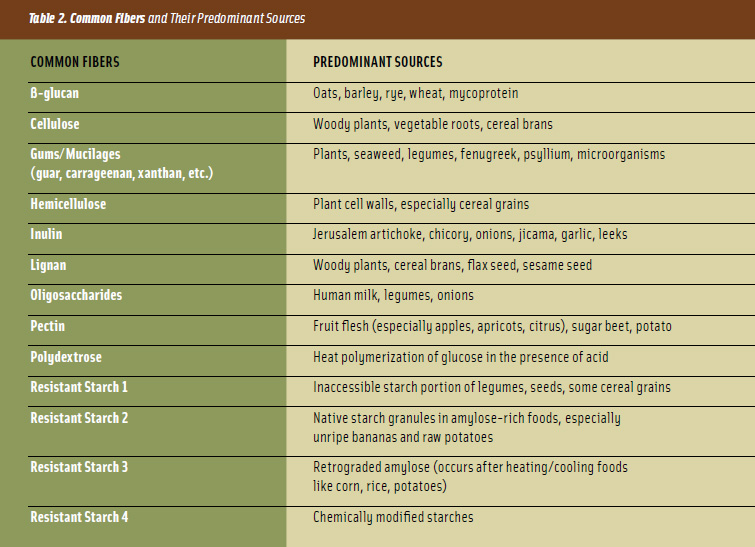
In the United States, dietary fiber intake is less than recommended, with usual intakes averaging only 15 g/day (DRIs, 2002). Many popular American foods are low in fiber, with servings of commonly consumed grains, fruits, and vegetables providing only 1 to 3 g of dietary fiber (Table 1). Legumes and high-fiber bread and cereal products supply more dietary fiber, but are consumed infrequently. Fibers can also be defined by their chemical or botanical components (Table 2). These descriptors become less useful as isolated fibers are chemically altered to improve functional properties. Knowing that a fiber source is a resistant starch, for example, tells you nothing about its physiological properties.
What Epidemiologic Studies Show
High intake of carbohydrates is linked to lower body weight. Saris (2003) reported an inverse relationship between carbohydrate intake and body mass index (BMI) in 8 of 9 studies. The "fiber hypothesis" suggests consumption of unrefined, high-fiber, carbohydrate-based foods protects against diseases - including diabetes, cancer, heart disease, and obesity - that are common in industrialized countries. However, this diet is both high in dietary fiber and low in dietary fat, making it difficult to separate out the cause of these beneficial effects. In epidemiologic studies, usual intake of dietary fiber, soluble fiber, and insoluble fiber can be measured and then linked to body weight.
--- PAGE BREAK ---
A multidisciplinary study of more than 5,000 individuals found that obesity was associated with increased energy intake and decreased consumption of fiber-rich foods like fruits and vegetables (Lissner et al., 1998). A longitudinal study found fiber intake was inversely associated with BMI at all levels of fat intake - even after adjustment for lifestyle factors and other confounding factors among young adults (Ludwig et al., 1999).
In the prospective Nurses Health Study, women who consumed more fiber consistently weighed less than women who consumed less fiber (Liu et al., 2003). Additionally, women in the highest quintile of dietary fiber intake had a 49% lower risk of major weight gain. Maskarinec et al. (2006) reported that plant-based foods and dietary fiber were most protective against excess body weight in a large, ethnically diverse population. Howarth et al. (2005) examined the association of dietary composition variables with BMI among U.S. adults ages 20 to 59 in the Continuing Survey of Food Intakes by Individuals (CSFII) 1994-1996. For women, a low-fiber, high-fat diet was associated with the greatest increase in risk of overweight or obesity compared with a high-fiber, low-fat diet. Davis et al. (2006) matched 52 normal-weight women to 52 overweight/obese women and found that the normal-weight subjects had higher fiber and fruit intake than the obese subjects.
Intervention Studies
Many intervention studies have been conducted to determine if dietary fiber intake assists in weight loss; the results have been inconsistent. In general, intervention studies are designed to monitor changes in body weight when subjects (either overweight or lean) are given low- or high-fiber diets. Birketvedt et al. (2000) found the addition of dietary fiber to a low-calorie diet significantly improved weight loss. The fiber-supplemented group lost 8.0 kg, while the placebo group lost only 5.8 kg. When postmenopausal women consumed higher-fiber diets as part of a study on very low-fat diets and weight loss, the women with higher fiber intakes lost significantly more weight (Mueller- Cunningham et al., 2003). A 12-week, randomized, controlled study of 34 individuals found that a high-carbohydrate diet consumed ad libitum (without energy restriction or change in energy intake) caused significant body weight and fat losses in older men and women (Hays et al., 2004).
Dietary Fiber and Energy Intake
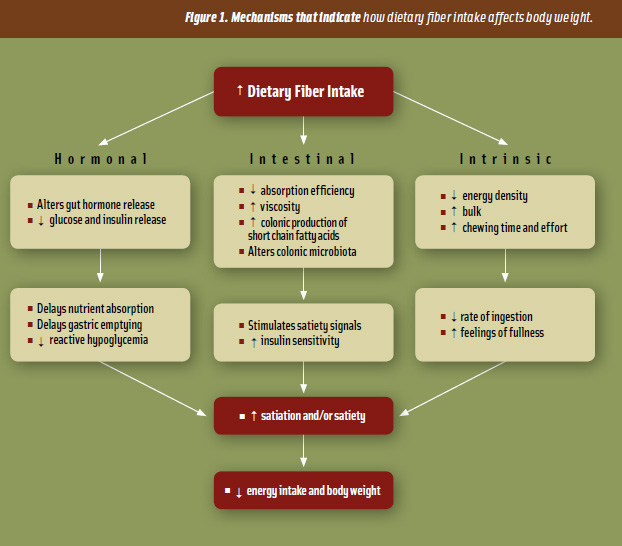
Heaton (1973) proposed that fiber acts as a physiological obstacle to energy intake through at least three mechanisms: 1) fiber displaces available calories and nutrients from the diet; 2) fiber increases chewing, which limits intake by promoting the secretion of saliva and gastric juice, resulting in an expansion of the stomach and increased satiety; and 3) fiber reduces the absorption efficiency of the small intestine.
Intrinsic, hormonal, and colonic effects of dietary fiber decrease food intake by promoting satiation and/or satiety (Figure 1). Examples of these controls include decreased gastric emptying and/or slowed energy and nutrient absorption. Gut hormone signaling also plays a significant role in satiety. Additionally, dietary fiber may also influence fat oxidation and fat storage.
Howarth and colleagues (2001) summarized the effects of dietary fiber on hunger, satiety, energy intake, and body weight. Most studies with controlled energy intake reported an increase in post-meal satiety and a decrease in subsequent hunger with increased dietary fiber. With ad libitum energy intake, the average effect of increasing dietary fiber across all the studies indicated that an additional 14 g of fiber/day resulted in a 10% decrease in energy intake and a weight loss of more than 1.9 kg through about 3.8 months of intervention. These effects were even more impressive in obese individuals. Increased dietary fiber - either from high-fiber foods or from fiber supplements - produced similar effects on weight regulation. Additionally, the beneficial effect of dietary fiber on weight regulation was seen for both soluble and insoluble dietary fiber. This group concluded that increasing the population mean dietary fiber intake from the current average of about 15 g/day to 25 - 30 g/day would be beneficial and may help reduce the prevalence of obesity.
--- PAGE BREAK ---
Fiber dose is an important consideration. Mattes (2007) compared a control breakfast bar to a breakfast bar containing alginate and guar gum (0.6 g fiber vs 4.5 g fiber) in obese subjects. No significant treatment effects or cumulative effects of satiety were found with the higher-fiber-containing bar. Oligofructose (16 g/day) taken in 2 doses increased satiety during breakfast (Cani et al., 2006). Total energy intake was 5% lower during the oligofructose treatment. Higher doses of alpha-cyclodextrin (a cyclic oligosaccharide) resulted in greater satiety than a control, but reduced palatability and increased gastro-intestinal complaints (Buckley et al., 2006). Overall, studies that report significant effects on satiety generally use larger doses of fiber.
Traditionally, high-fiber foods have been solid foods. However, some of the newer functional fibers, such as resistant starches and oligosaccharides, can be easily added to drinks and may not alter viscosity. Few studies on the satiating effects of drinks supplemented with these soluble, non-viscous fibers have been published. Moorhead et al. (2006) compared test lunches with 200 g of whole carrots, blended carrots, or carrot nutrients. Whole carrots and blended carrots resulted in significantly higher satiety. Ad libitum food intake for the remainder of the day decreased in this order: carrot nutrients, blended carrots, whole carrots. The researchers concluded that both fiber content and food structure are important determinants of satiety. A similar study was conducted using apples, applesauce, and apple juice (with added fiber) as a pre-load before a meal. Although the three foods contained the same calories and fiber, subjects ate significantly less lunch when consuming the whole apple compared with the applesauce, apple juice, or no pre-load. Again, this suggests that adding fiber to a beverage may not necessarily enhance satiety - and that solid foods may be more satiating than liquids (Flood and Rolls, 2007).
Many studies support that increased dietary fiber intake promotes satiety and decreases hunger and thus helps provide a feeling of fullness (Slavin and Green, 2007). Satiation is defined as the satisfaction of appetite that develops during the course of eating and eventually results in the cessation of eating. Satiety refers to the state in which further eating is inhibited and occurs as a consequence of having eaten. Fiber-rich foods tend to have a high volume and a low energy density and should promote satiation and satiety. Rolls (2000) suggested humans might consume a constant weight of food. If this is true, then a constant weight of lower-energy food (i.e. high fiber) may promote a reduction in body weight by displacing energy or calories from foods with greater energy density, such as high-fat foods. The bulking and viscosity properties of dietary fiber are predominantly responsible for influencing satiation and satiety (Burton-Freeman, 2000).
Research on how different types of fiber affect appetite, energy, and food intake has been inconsistent. Results differ according to the type of fiber and whether it is added as an isolated fiber supplement or naturally occurring in a food. Short-term studies that assess energy intake after subjects are fed fiber-containing meals suggest large amounts of total fiber are most successful for reducing subsequent energy intake. Higher-viscosity fibers appear most successful in promoting satiety, while new, soluble fibers appear to have minimal effects on satiety, even if consumed in very large doses (Slavin and Green, 2007). Longer-term studies that examine how both intrinsic and functional fibers impact satiety are required, yet there is ample evidence to suggest that increasing consumption of high-fiber foods - especially viscous fibers - may decrease feelings of hunger by inducing satiation and satiety. Table 3 lists fibers that have been found to decrease energy intake.
--- PAGE BREAK ---
Gut Hormones and Satiety
The organs of the gastrointestinal tract have an important role in sensing and signaling the regulation of energy homeostasis. The gut uses neural and endocrine pathways to communicate and control energy balance. Gut peptides play an important role in the regulation of food intake and energy homeostasis (Murphy et al., 2006). Many hormones have been associated with decreasing appetite and food intake, while only one "ghrelin" is known to stimulate the appetite. The relationship between gut hormones and satiety is highly complex. For example, gut hormone release, and effectiveness, is largely dependent on body weight, gender, receptor status, amount of food consumed (i.e. 100 calories vs 1,000 calories) and type of food intake (i.e. fiber, fat, carbohydrate, protein). The specific role of individual gut hormones is currently under investigation, though it is clear that complex interactions between these peptides play a role in appetite regulation.

Few gut hormones have been measured with a fiber question in mind. Gruendel et al. (2006) reported that acylated ghrelin was lowered with the addition of carob fiber to a liquid meal. However, carob fiber is also high in polyphenolic compounds that may be responsible for altered ghrelin levels. Erdmann et al. (2006) reported differences in ghrelin response between normal and obese subjects. Arabinoxylan, a soluble fiber, was fed to 11 subjects with normal glucose metabolism (Mohling et al., 2005). Glucose response was not significantly different in subjects; however, plasma ghrelin was higher two hours after the fiber than after the control meal.
Fiber and the Future
Modest increases in consumption of fruits, vegetables, legumes, and whole and high-fiber grain products would bring the majority of North American adults close to achieving the dietary fiber recommendations of 14 g/1,000 kcal. In addition, a higher fiber intake provided by foods is likely to be less calorically dense and lower in fat and added sugar. All efforts should be made to maintain the fiber content of processed foods and enhance the fiber content of foods naturally low in fiber. It must be stressed, however, that dietary fiber sources are not equally effective in reducing food intake and improving satiety. Isolated or functional fibers should be tested in human subjects before claims are made about physiological effectiveness for weight maintenance.
This article is based on a paper presented at the 2007 IFT Annual Meeting & Food Expo, Chicago, Ill., July 28-August 1.
References
Birketvedt, G.S., Aaseth, J., Florholmen, J.R., and Ryttig, K. 2000. Long-term effect of fibre supplement and reduced energy intake on body weight and blood lipids in overweight subjects. Acta. Medica. 43: 129-132.
Buckley, J.D., Thorp, A.A., Murphy, K.J., and Howe, P.R. 2006. Dose-dependent inhibition of the post-prandial glycaemic response to a standard carbohydrate meal following incorporation of alpha-cyclodextrin. Ann. Nutr. Metab. 50: 108-114.
Burton-Freeman, B. 2000. Dietary fiber and energy regulation. J. Nutr.130: 272S-275S.
Cani, P.D., Joly, E., Horsmans, Y., and Delzenne, N.M. 2006. Oligofructose promotes satiety in healthy human: a pilot study. Eur. J. Clin. Nutr. 60: 567-572.
Davis, J.N., Hodges, V.A., and Gillham, M.B. 2006.Normal-weight adults consume more fiber and fruit than their age- and height-matched overweight/obese counter-parts. J. Am. Diet. Assoc. 106: 833-840.
Erdmann, J., Leibl, M., Wagenpfeil, S., Lippl, F., and Schusdziarra, V. 2006. Ghrelin response to protein and carbohydrate meals in relation to food intake and glycerol levels in obese subjects. Regulatory Peptides 135: 23-29.
Flood, J.E. and Rolls, B.J. Does Consuming Fruit in Different Forms Affect Food Intake and Satiety? [Oral Presentation and Abstract]. NAASO 25th Annual Scientific Meeting, 2007, New Orleans, La.
Gruendel, S., Garcia, A.L., Otto, B., Mueller, C., Steiniger, J., Weickert, M.O., Speth, M., Katz, N., and Koebnick, C. 2006. Carob pulp preparation rich in insoluble dietary fiber and polyphenols enhances lipid oxidation and lowers postprandial acylated ghrelin in humans. J. Nutr. 136: 1533-1538.
Hays, N.P., Starling, R.D., Liu, X., Sullivan, D.H., Trappe, T.A., Fluckey, J.D., and Evans, W.J. 2004. Effects of an ad libitum low-fat, high-carbohydrate diet on body weight, body composition, and fat distribution in older men and women. Arch. Intern. Med. 164: 210-217.
Heaton, K.W. 1973. Food fibre as an obstacle to energy intake. Lancet. 2: 1418-1421.
Howarth, N.C., Saltzman, E., and Roberts, S.B. 2001. Dietary fiber and weight regulation. Nutr. Rev. 59: 129-139.
Howarth, N.C., Huang, T.T.K., Roberts, S.B., and McCrory, M.A. 2005. Dietary fiber and fat are associated with excess weight in young and middle-aged U.S. adults. J. Am. Diet. Assoc. 105: 1365-1372.
Institute of Medicine of the National Academies. 2002. Dietary Reference Intakes: Energy, Carbohydrates, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids., The National Academies Press, Washington, D.C., USA.
Lissner, L., Lindroos, A.K., and Sjostrom, L. 1998. Swedish obese subjects (SOS): An obesity intervention study with a nutritional perspective. Eur. J. Clin. Nutr. 52: 316-322.
Liu, S., Willett, W.C., Manson, J.E., Hu, F.B., Rosner, B., and Colditz, G. 2003. Relation between changes in intakes of dietary fiber and grain products and changes in weight and development of obesity among middle-aged women. Am. J. Clin. Nutr. 87: 920-927.
Ludwig, D.S., Pereira, M.A., Kroenke, C.H., Hilner, J.E., Van Horn, L., Slattery, M.L., and Jacobs, D.R. 1999. Dietary fiber, weight gain, and cardiovascular risk factors in young adults. JAMA 282: 1539-1546.
Maskarinec, G., Takata, Y., Pagano, I., Carlin, L., Goodman, M.T., Le Marchand, L., Nomura, A.M.Y., Wilkens, L.R., and Kolonel, L.N. 2006. Trends and dietary determinants of overweight and obesity in a multiethnic population. Obesity 14: 717-726.
Mattes, R.D. 2007. Effects of a combination fiber system on appetite and energy intake in overweight humans. Phys. & Behaviour 90: 705-711.
Mohling, M., Koebnick, C., Weickert, M.O., Lueder, W., Otto, B., Steiniger, .J, Twilfert, M., Meuser, F., Pfeiffer, A.F.H., and Zunft, H.J. 2005. Arabinoxylan-enriched meal increases serum ghrelin levels in healthy humans. Hormone and Metabolic Res. 37: 303-308.
Moorhead, A.S., Welch, R.W., Livingstone, B.M., McCourt, M., Burns, A.A., and Dunne, A. 2006. The effects of the fibre content and physical structure of carrots on satiety and subsequent intakes when eaten as part of a mixed meal. Br. J. Nutr. 96: 587-595.
Mueller-Cunningham, W.M., Quintana, R., and Kasim-Karakas, S.E. 2003. An ad libitum, very low-fat diet results in weight loss and changes in nutrient intakes in postmenopausal women. J. Am. Diet. Assoc. 103: 1600-1606.
Murphy, K.G., Dhillo, W.S. and Bloom, S.R 2006. Gut peptides in the regulation of food intake and energy homeostasis. Endoc. Rev. 27: 719-727.
Rolls, B.J. 2000. The role of energy density in the overconsumption of fat. J. Nutr. 130 (2 suppl): 268S-271S.
Saris, W.H.M. 2003. Glycemic carbohydrate and body weight regulation. Nutr. Rev. 61: S10-S16.
Slavin, J.L.2005. Dietary fiber and body weight. Nutrition 21: 411-418.
Slavin, J.L., and Green, H. 2007. Fibre and satiety. Nutrition Bulletin 32 (Suppl 1): 32-42.
Authors
-
JOANNE SLAVIN, ABBY KLOSTERBUER, , HOLLY WILLIS
Categories
-
Food Health Nutrition
-
Food Categories
-
Food Ingredients and Additives
-
Functional Foods
-
Obesity and Weight Management
-
Carbohydrate
-
Grains
-
Food Technology Magazine


